The story starts with a surgeon who must have been tired of describing procedures to patients. He put up a hand to stop my questions at the first visit, when he laid out a plan that ultimately involved straightening my fingers.
However when he said this process would take 3 operations that was the end of the road. With a full time job I could not afford the time to have that much surgery. His plan was to fuse both wrists and then straighten the fingers - I found out on my own that this is the best way to proceed. His explanation of his reasoning was not 'patient-friendly.'
Once I retired I was able to take the time to start with surgeries. The results of operation #1 were very successful, so after a year I went back to have a second wrist fusion. With both wrists immobilized and with the new found ability to turn my hand palm up, I was ready for the grand finale and just in time, because my fingers were getting worse and using them was getting more difficult.
How much worse? This much
But - when I went back to the surgeon, he said "Too bad you didn't have this done when I suggested it because I'm retiring." Not the most sympathetic doctor, but also not the only one in the city.
Now it's done and I have new knuckles. Despite telling Debby's story of success with this I had doubts, especially when a trusted friend told me that doctors in her city were no longer willing to do this procedure.
However, with a US friend who has RA finding that three of her fingers were so badly displaced that she has lost hand function I carried on.
This is a picture of what I believe my knuckles look like on X-ray now. I don't have an x-ray of my own since the doctor did not do one. Now I have an implant in all 4 of my knuckles (MCP joints).

Silastic implants
You might wonder whether the operation was a success.
It was done ten weeks ago. I started in a cast, then graduated to various splints. Every week the Occupational Therapist would adjust both the night splint and the one I wore during the day.
The day splint became smaller as I was able to gradually start moving my joints more and to start on a gradually increasing exercise program. I felt that the splinting and the exercise program were as important to the operation's success as the surgery.


It was done ten weeks ago. I started in a cast, then graduated to various splints. Every week the Occupational Therapist would adjust both the night splint and the one I wore during the day.
The day splint became smaller as I was able to gradually start moving my joints more and to start on a gradually increasing exercise program. I felt that the splinting and the exercise program were as important to the operation's success as the surgery.


Now I am able to write again and to type faster. The occupational therapist who is still helping me advised me to wear a small splint to keep my fingers straight during the day, and a splint from fingertips to forearm at night. In retrospect I think that the surgery was only half of the procedure - occupational therapy and dynamic splinting was vital for the final success.
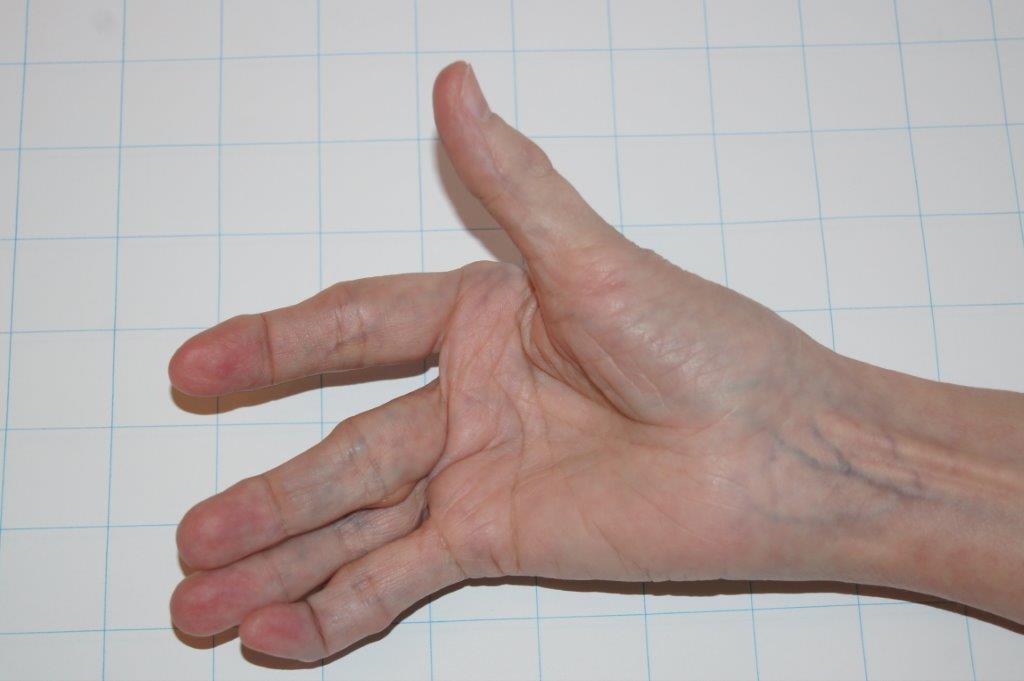
Here's the finished product - my hand today! Better than before.

It's a perfect example of the teamwork between professionals that is required for the best results to patients.
Perfection is impossible, but I expect to be able to use my hand for a lot more years now, and better long-term function was the main reason I had the surgery.
Perfection is impossible, but I expect to be able to use my hand for a lot more years now, and better long-term function was the main reason I had the surgery.

